WEISS 2014 投射认同的五阶段模型 - 7

王静华2016-4-21 15:22
查看:2931次
王静华:第三、第四和第五个阶段
Third phase: Linking the projection with an internal object of the analyst
第三个阶段:投射与分析师内部客体的联结
According
to I. Brenman Pick (1985) the patient “does not just project
into the analyst” (p. 49), but endeavours at all times to place his projections
into specific aspects of the analyst. “A spontaneous emotional
reaction” (p. 52) takes place with the projections of
the patient, which is an experience which, according to her, will be most
useful for interpreting when it is fully and wholly respected and not overly
ruled by the demand of absolute neutrality. The penetrating projection has a
tendency to connect to an internal object of the analyst. If this connection
fails or alternatively when there is an adhesion to the analyst’s own
non-assimilated psychotic anxieties, the penetrated projection will be
experienced like a foreign body in the countertransference (for example, in a
countertransference dream with psychotic elements) or as something that
threatens to swamp the analyst. If the connection is too tight/closely fitting,
the patient will become an internal object for the analyst, as it were, as
described by Money-Kyrle (1956). The type of readiness for
either a concordant or complementary countertransference reaction depends on
whether the projection originated in a part of the self or in an internal
object of the patient (Racker, 1953, 1980). However, frequently the projections
will encompass both aspects so that it activates a part of the self or an
internal object simultaneously or in turn.
布兰曼·皮克(1985)认为病人“并不仅仅是投射进分析师”(p.49),而且一直竭力将他的投射置放进分析师特定的特征内。病人的投射会自然而然地引发情感反应,皮克认为,这种情感体验被充分完全地尊重时就可以形成非常有用的解释,而不是被绝对中立的需要过度支配。这种渗透投射趋向于连接分析师的内部客体。如果当联结失败或者依附到分析师自身的非-吸纳性的精神病性元素,渗透投射就会在反移情中被体验为来自外部实体(例如,带有精神病性元素的反移情的梦)或者是某些会淹没分析师的危险。如果连接太紧/紧密扣合,病人就似乎成为分析师的过去的一个内部客体,蒙利·凯里(1956)。这种类型可能是一致性反移情或者是补偿性反移情,这取决于投射源于病人的部分自体还是病人的内部客体(拉克尔,1953,1980)。可是,投射常常是包含两者的,因此它可能同时激活部分自体或者内部客体,或者轮流激活。
A patient described such a situation when she said that she experienced the sessions with me as “sugar hours”. In such instances, she ignored the content of my interpretations and was solely identified with the sound of my voice, at times even getting me to speak in a particularly soft and appeasing way. At other times, she only heard the content of my words, which she experienced as accusatory, merciless and cruel. On the one hand I seemed to be identified with an idealized part of herself, on the other I was identified with a cruel internal object. As long as we maintained this constellation and I felt guilty, we were in a gridlock in which there was either tenderness or cruelty, ‘love without words’ or ‘words without love’, but no room for separateness, development or thinking.
一个病人说她将与我的会谈体验为“甜蜜时刻”。在这种情况下,她忽略我给出的解释内容,唯独与我的声音认同,有时甚至迫使我不得不以一种特别温柔和安抚性的方式说话。其他时候,她只听我话语中的内容,并体验为指责的、无情的、残酷的。一方面,我看起来被认同为她理想化的部分,另一方面,我被认同为一个残酷的内部客体。只要我们维持这种序列,我对此感到内疚,我们处于一个僵局,要么是温柔的要么是残酷的,要么是“有爱没有话语”要么是“有话语就没有爱”,没有空间可以分离、推进或者是思考。
Meltzer (1966, 1992) pointed out that the projective identification does penetrate the internal objects and modify them momentarily or permanently. The kind of connection which now develops between the projected parts of the patient and the internal world of the analyst will decide how the analyst experiences ‘the patient in him’ in the countertransference and whether he will be able to release himself from identification and the patient’s internal objects. It is only when he can regain an observational stance vis-a-vis the feelings evoked in him and compare them with the material from the patient that he will be in a position to use his countertransference as an aid rather than being ruled by it (Segal, 1997, p. 119). If he is ‘swamped’ by the projection he will not be able to think about it, but will endeavour to rid himself of it as in the example of Bion.
梅尔兹(1966,1992)指出投射认同并不会渗入内部客体,暂时或永久地更改它们。现在,病人投射部分和分析师内部世界之间发展起来的这种联结,将会决定分析师如何以反移情的方式体验到“在他内部的病人”,以及是否能够从认同和病人的内部客体中解放自己。只有当分析师重回观察位以及觉察到他内在被诱发的感觉,与来自病人的材料进行对比,这样他就处在使用他自己的反移情的位置上,而不是被反移情所支配。如果分析师被投射所“淹没”,他将没有能力对此进行思考,反而会竭力摆脱投射,就像比昂的那个例子一样。
Fourth phase: Transformation of the projection
第四个阶段:投射的转化
The next
step will deal with the transformation of the projection into a comprehensible
form. That means that the analyst will attempt unconsciously to compare the
projected elements with familiar experiences and to ‘read’ them using other
internal objects and functions (see Figure 3). Similar processes were described
by representatives of the mentalization theory(心理化理论) as ‘reflexive function’( 反思功能) (Fonagy and Target, 1997) or as ‘affect modulation’ (情感调谐)in the intersubjective matrix(主体间性母体或者主体间性基质,殷一婷:不可翻译为主体间空间,主体间可能有空间,也可能没有空间,也可能是各种形式和状态) of early childhood (Gergely and Watson, 1996).
这一步就是将投射转化为可以被理解的形式。意味着分析师将在无意识中尝试着把投射的元素与熟悉的体验比对,并使用其它内部客体和功能“读出”它们(见图3)。对这个过程其它类似的描述包括“心理化理论”中的“反思功能”(冯纳吉 & 塔吉特,1997)或者是幼儿时期主体间性母体的“情感调谐”。
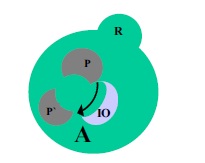
Fig. 3. Transformation of the projection through comparison with the internal objects (IO) of the analyst
图3
通过和分析师内部客体(IO)的对比,转化投射
In this
context, the focus is put on the intrapsychic processes evolving in the
analyst because they are clinically the most relevant aspects. In order to be
able to “read” these elements projected by the patient, he has to be able to
differentiate these, step-by-step, from similar but not identical parts of his
own self (Steiner, 1996, p. 1080). This work will become all the more difficult
the more the projected elements correspond to an uncomprehended or ‘difficult’
area in his own internal world. This internal process in the analyst comprises
different sequences which have not been investigated sufficiently.
对此,焦点就放在分析师内不断演化的心灵内过程,因为这些过程是在临床上最有意义的特征。为了能够“读出”病人投射的元素,他需要有能力,一步一步地,区分出这些相似的但并不是他自体的构件元素(斯坦纳,1996,p.1080)。投射元素越是接近分析师自己内在世界中未被理解或是“困难”的区域,这个区分的工作就愈加的困难。而这个内在世界的过程包含不同的单独的系列事件,它们尚未被充分探索过。
These include identification with a good internal parental couple (Heimann), reparation of the analyst’s own damaged internal objects (Money-Kyrle) and a capacity for symbol formation (Segal).4 The projections of the patient can be modified and transformed into a more intelligible form, if it were possible to establish an internal triangulation to some degree. Bion (1962b) described this process as a-function. Sandler and Sandler (1984; Sandler, 1976) refer to a similar process in describing the ‘free-floating role-responsiveness’ of the analyst, which allows him to absorb as well as reciprocate the object relationships ‘brought about’ by the patient.
这些包括认同内在好的父母联合体(海曼),修复分析师自身受损的内部客体(蒙利·凯里)和象征形成的能力(西格尔)。如果有可能在一定程度上建立起这样内在的三角关系,病人的投射就能够被修改并转化为更易理解的形式。比昂(1962b)将这个过程描述为阿尔法功能。桑德拉和桑德拉((1984; 桑德拉, 1976)提到分析师的“不同角色回应间的自由浮动”是类似的过程,这使得分析师可以吸收、也可以修复病人“唤起”的客体关系。
Pathology
病理学
If the
transformation does not succeed, the projection either gets stuck as a ‘bizarre
object’ in the internal world of the analyst (haunting him like an alien body
or ‘concrete’ thought in his psyche) or else forms a permanent alloy with an internal object of the analyst and thus
creates pressure, which he would like to be rid of in one way or another (e.g.
through defensive measures, hidden acting out or defensive re-projection). This
situation was described by Grinberg (1962; 1990, pp. 83–5) as “defensive counter-identification”. Its
equivalent would be the classic countertransference neurosis.
如果转换没有继续,投射被卡在分析师的内在世界里、就像一个“匪夷所思的客体”(就像一个诡异实体般缠绕着分析师或者在他的精神里“固结”思考),或者和分析师内部形成了一个永久的联合体、进而制造压力,使得分析师想要以这种或那种方式摆脱它(例如,通过防御性方式,隐蔽的付诸行动或者是防御性的再投射)。格林伯格(1962; 1990, pp. 83–5)称之为“防御性的反-认同”,等同于典型的反移情神经症。
However,
if one deals with a limited and transient reaction, such enactments can in turn become starting points for further
understanding (Feldman, 1997; Joseph, 1989; Steiner, 2006b), if the analyst
manages to disengage himself from the entanglement he got himself into (see
Hinz, 2003). Such micro-processes seem at times unavoidable, particularly in
the treatment of borderline patients and can be understood as part of the
analyst’s unconscious working through of primitive object relations. Gabbard (1995)
in particular has pointed out the connections between the concept of enactment
as developed by ego psychology (Jacobs, 1986, 2001) and the actual
Kleinian view of projective identification.
可是,如果只是有限且短暂的反应,如果分析师设法让自己从陷入的缠绕中解脱出来,这种付诸行动反而成为进一步理解的起始点(费尔德曼, 1997; 约瑟夫, 1989; 斯坦纳, 2006b)。这样的细微过程有时是很难避免的,尤其是治疗边缘性病人,可以理解为是分析师原始客体关系无意识的部分修通。加博德(1995)特别指出自我心理学的付诸行动的概念和克莱因学派的投射认同概念之间的联系。
Fifth phase: Interpretation and re-projection
第五个阶段:解释和再投射
If the
analyst is able to work with the absorbed projection, that is, to distinguish the
projection from his own internal objects, it can be re-introjected in its
modified form (Money-Kyrle) and taken back by the patient (see Figure 4).
如果分析师能够与被吸收的投射工作,也就是能够从他自己的内在客体中区分出投射的部分,投射就能够被以修改后的形式再摄(蒙利·凯里)并被病人收回(见图4).
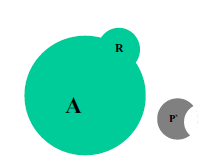
Fig. 4. Re-projection of the transformed projection
图4
投射转化后的再投射
This
form of re-projection is non-defensive. It is different from other forms of
re-projection, which the analyst might use to maintain his internal equilibrium
or rather to rid himself of something unbearable (see Feldman, 1997). The
benign form of re-introjection will trigger a cycle of understanding, while the
defensive forms of re-introjection might set off a malignant ‘cycle of misunderstanding’ in certain circumstances (Weiss, 2003b). The former can, for example, be
brought about through the use of analyst-centred interpretations (Steiner,
1993), which will convey a feeling of containment, and which initially only aim
to examine the function of the picture the patient is generating of the analyst
at any one moment of the analysis. At a later stage, the analyst can then go on
to patient-centred interpretations. In the case of escalating misunderstanding
defensive re-projections may be embedded into the patient’s defensive
organization (Mitrani, 2009)
这种形式的再投射是非防御性的。不同于其他形式的再投射,此时分析师通常是维持了他内在的平衡而不是去摆脱某些他无法忍受的(费尔德曼,1997)。好的再摄将触发一系列的理解,而防御性的再摄可能在某些情境下引发有害的“误解循环”(韦斯,2003b)。例如,前者可以通过使用分析师-中心的解释带来(斯坦纳,1993),这传达了一种包容性的感觉,这原本仅仅是为了核对病人头脑中的影像的功能,这个影像是病人针对分析师、在分析的任何时刻产生的。在更有进展的阶段,分析师就可以继续病人-中心解释。对防御性投射的持续攀增的误解可能嵌入进病人的防御系统内(玛崔尼,2009)。
译者注
P133 JOHN
STEINER 1993《Psychic Retreats Pathological Organizations in
Psychotic, Neurotic and Borderline Patients》 Chapter 11:Problems of
psychoanalytic technique: patient-centred and analyst-centred interpretations
…… Some analysts, in these circumstances, tend to phrase
their interpretations in a form which recognizes that the patient is more interested
in what is going on in the analyst’s mind than in his own. At these times the
patient’s most immediate concern is his experience of the analyst, and this can
be addressed by saying something like, ‘You experience me as…’, or ‘You are
afraid that I…’, or ‘You were relieved when I…’, or ‘You became anxious a
moment ago when I …’. I think of such interpretations as analyst-centred and
differentiate them from patient-centred interpretations, which are of the
classical kind in which something the patient is doing, thinking, or wishing is
interpreted, often together with the motive and the anxiety associated with it.
In general, patient-centred interpretations are more concerned with conveying
understanding, whereas analyst-centred interpretations are more likely to give
the patient a sense of being understood…….
…在这种情况下,一些分析师倾向的解释的措辞形式会认为病人对分析师头脑中的想法相比病人自己的更加感兴趣。在这种时候,病人最直接关注的是他所体验到的分析师,这时的表达方式就类似于,“你体验到我就像…”, “你担心我会…”,“当我…你感到轻松”,“刚才当我…你变得焦虑起来”。我认为这样的解释就是 分析师-中心,不同于病人-中心的解释,解释就是典型的那种病人正在做什么、想什么,或者是愿望,通常还同时给出动机和与之有关的焦虑。总而言之,病人-中心的解释更加关注传达理解,而分析师-中心解释更有可能给让病人有被理解的感觉…
(待续...)